Enterprise AI-Powered Platform for Life Sciences
Digitize Quality, Lab & Manufacturing
APQR | CPV | LIMS | QMS | Compliance
at
PHARMAP 2026
AmpleLogic will be attending PHARMAP 2026, the Pharmaceutical Manufacturing & Packaging Congress, in Amsterdam on April 20–21, 2026.
Visit us at Booth No. 13 to explore our aPaaS-based solutions for digital transformation, compliance, and quality management in the life sciences industry.
Years
Innovation in Pharma Digitalization
Clients
Globally Satisfied
GAMP Solutions
COTS Applications
Qualified Engineers
Dedicated Validation Team
Happy Users
Global Footprint
Why Siloed Pharma Software Is Costing You More Than You Think
Most pharma companies run 5-10 disconnected platforms for quality, lab, manufacturing, and compliance. The hidden costs add up fast.
Siloed QA, QC & manufacturing workflows delay batch release
Disconnected systems force manual hand-offs between quality, lab, and production -- adding days to every batch cycle.
Up to 30% longer batch release times
QA/QC workloads keep rising despite existing eQMS, DMS & LIMS
Point solutions don't talk to each other. Teams re-enter data, chase approvals, and compile reports manually.
40%+ time spent on non-value work
Legacy platforms make every process change slow and expensive
Rigid architectures require vendor tickets and paid consultants for even minor workflow updates.
6-12 month change cycles
Growing demand for traceability, audit readiness & data intelligence
Regulators expect real-time visibility. Spreadsheets and fragmented databases can't deliver it.
Recurring audit findings
Increasing product complexity -- biologics, CGT & global supply chains
New modalities require flexible, connected systems that legacy COTS platforms weren't designed for.
Higher compliance risk
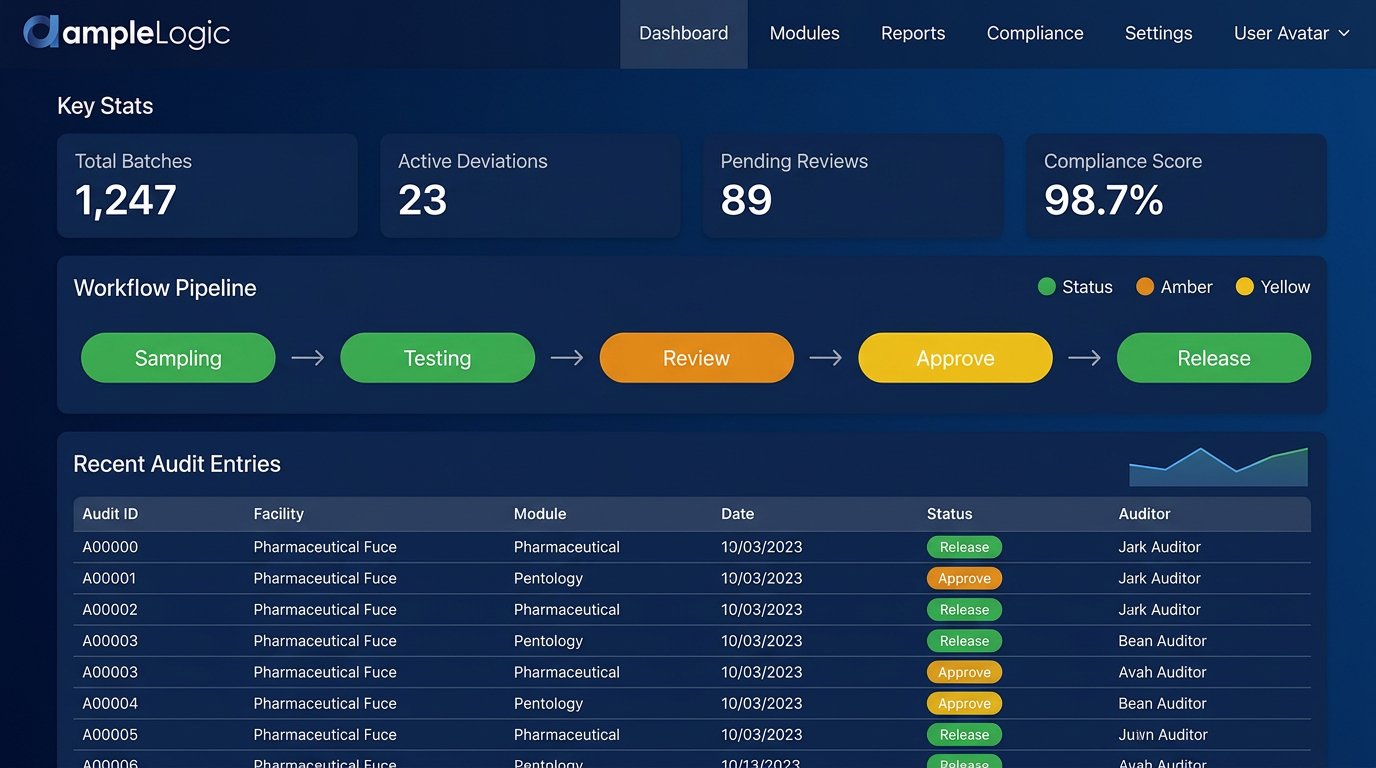
Introducing APQR & CPV for GMP Manufacturing
AmpleLogic now delivers Annual Product Quality Review (APQR) software and Continued Process Verification (CPV) software on one unified platform — replacing manual PQR processes, Minitab charting, and disconnected spreadsheets with automated, AI-driven quality intelligence.
Annual Product Quality Review Software
Cloud-based APQR software that automatically aggregates manufacturing, quality, and laboratory data across LIMS, eQMS, MES, ERP, and DMS to generate compliant PQR reports, Quality Management Reviews (QMR), and regulatory-ready dossiers — delivering real-time pharmaceutical product quality review insights and process capability analytics.
70–80%
APQR Prep Time Reduction
Zero
Manual Data Compilation
6σ
Statistical Reports
- Automated PQR report generation with configurable APQR templates by product type, site, and regulatory market
- Built-in Six-Pack reports, Cp/Cpk/Pp/Ppk analysis, and Nelson Rule detection — replaces Minitab, SAS, and SPSS
- AI-powered summary narratives, OCR data extraction, and 5 Whys root cause analysis for faster report completion
- Cross-system data aggregation from LIMS, eQMS, MES, DMS, ERP, Stability, and Calibration systems
- Batch-wise trending, CPK visual indicators, and process parameter comparison reports for continuous quality monitoring
- GMP compliant with FDA, EMA, MHRA, WHO, ICH Q7, and ICH Q10 — 21 CFR Part 11 and Annex 11 ready
Continued Process Verification Software
Digital CPV software for pharmaceutical manufacturing that transforms continued process verification from manual statistical monitoring into an AI-driven manufacturing intelligence platform — predicting deviations, optimizing processes, and ensuring consistent product quality across the validation lifecycle (Stage 1, 2, and 3).
Real-Time
CPP/CQA Monitoring
75%
Effort Reduction
100%
Audit Trail Coverage
- Real-time monitoring of Critical Process Parameters (CPPs) and Critical Quality Attributes (CQAs) across all manufacturing operations
- Automated SPC charting — I-MR, X-bar R, control charts with Nelson Rule violation detection and capability index tracking
- R-based statistical engine for Six-Pack reports, ANOVA, regression, and multivariate analysis — no manual Minitab exports
- Predictive AI analytics that detect process drift before batch failures, with automated trend interpretation and anomaly detection
- Seamless APQR integration — Stage 3 CPV evidence automatically populates annual product quality reviews
- Compliant with FDA Process Validation Guidance, ICH Q8/Q9/Q10, EU GMP Annex 15, and 21 CFR Part 11
Unified APQR + CPV Platform
Unlike standalone tools, AmpleLogic delivers both annual product quality review and continued process verification on a single platform with shared data, shared analytics, and shared compliance — eliminating data silos between Stage 3 monitoring and annual quality reviews.
One Low-Code Pharma Platform Replaces 14+ Siloed GMP Software Vendors
Instead of buying separate LIMS, eQMS, MES, DMS, and LMS from different vendors -- deploy them all on a single extensible platform with shared data, shared workflows, and shared compliance.
Visual Low-Code Builder
Drag-and-drop tools to build, customize, and deploy GxP applications -- no custom coding required.
Configurable Workflow Engine
Multi-level approvals, electronic signatures, and audit trails out of the box. Change workflows in hours, not months.
Single Unified Data Layer
One database powering all 14+ modules. Zero point-to-point integrations. Real-time data sharing across quality, lab, and plant.
Built-In GxP Compliance
Pre-validated against 21 CFR Part 11, Annex 11, GAMP 5, and EU GMP guidelines from day one.
Any Device, Anywhere
Responsive interfaces that work on shop floor tablets, lab desktops, and executive phones.
Open Integration Framework
REST APIs, HL7, SAP, and 50+ pre-built connectors to plug into your existing ERP and instrument ecosystem.
AI Solutions for Pharma Digitalization
Automate processes and strengthen compliance across document management, reporting, SOPs, and CAPA.
AI-Powered Document Management
Chatbot UI, automated indexing, and regulatory-ready audit trails for faster retrieval and consistent records.
Faster retrieval, consistent records, and audit readiness
Agentic AI Report Builder
Automated report generation and context-aware summaries for QC and leadership teams.
Reduce manual reporting time and improve oversight
AI Recommendation Engines
Root-cause suggestions for deviations and CAPA, with prioritized actions for faster resolution.
Data-driven prioritization to shorten resolution cycles
SOP Podcast & Employee Evaluation
Automated question generation and SOP podcast in multilingual for training and engagement.
Generate MCQs with plausible distractors and detailed explanations for effective knowledge evaluation
From Concept to Compliance in Three Steps
Consult & Define
Our domain experts map your workflows, compliance requirements, and integration needs to create a tailored deployment blueprint.
Configure & Validate
Using our low-code aPaaS, we configure pre-validated modules to your exact specifications. No custom coding, no compliance gaps.
Deploy & Scale
Go live in weeks, not months. Our team handles training, data migration, and post-go-live support to ensure a seamless transition.
Results That Speak for Themselves
Time-to-Market Acceleration
Rapid rollout of QA, QC, Manufacturing, and Regulatory systems using low-code pharma components.
Reduction in Integration Costs
All applications built on a single platform offer ready integrations, reducing integration costs significantly.
Savings in Infrastructure Costs
Adoption of open-source servers like Linux and PostgreSQL cuts infrastructure costs dramatically.
Regulatory Compliance
Compliance with US FDA and MHRA; CFR Part 11 and Annex 11 built into every module from day one.
Project Success Rate
Vs 54% IT industry average, showcasing superior delivery consistency across 500+ implementations.
Domain Expertise
Deep Life Sciences knowledge embedded in every product. We understand GxP, 21 CFR Part 11, and Annex 11.
Commitments That Drive Adoption
Two pillars that accelerate learning, repeat business, and lower ownership costs
Technology and Talent
Proactive adoption of emerging technologies to enable employee learning and secure market leadership.
Product Innovation and TCO
Continuous product updates that streamline integrations and minimize total cost of ownership.
From 120+ Pharma Customers to Proven Repeat Business
Selected repeat engagements demonstrating trust, compliance, and faster ROI across pharma and biotech.






















ISO 9001:2015
Quality Management
ISO 27001:2022
Information Security
SOC 2
Compliant
Recognized by Industry Analysts
Verified G2 rating 4.8/5 from 300+ Reviews
Frost & Sullivan
Leader Quadrant Recognition 2025
AmpleLogic positioned in Leader quadrant for life sciences LIMS 2025.
Gartner
RIMS 2024 Evaluation Cycle
Validates vendor viability and product maturity for enterprise buyers.
Markets & Markets
Top 16 Global QMS 2025
Listed in 16 top global pharmaceutical quality management software (QMS).
Gartner
LIMS 2025 Evaluation Cycle
AmpleLogic positioned in Leader quadrant for life sciences LIMS 2025.
"Rapid implementation and intuitive drag-and-drop builder delivered accelerated, compliant app delivery with ROI in months."
"Responsive customer service and pre-validated components accelerated our audit readiness and reduced compliance risk across implementations."
"Customers report faster validation, stronger compliance, and measurable ROI following adoption."
89 G2 Badges. 291+ Verified Reviews.
AmpleLogic is recognized as a Leader and High Performer across Medical QMS, Document Management, Healthcare LMS, and more on G2 — the world's largest software review platform.
G2 Badge Highlights — Summer 2024
What Customers Say on G2
"Amplelogic QMS system has all the required quality related modules and all the deviations, change controls and CAPA's are effectively maintained and tracked. All the modules are super easy to use."
Kandikattu K.
Quality Professional
"It gets integrated with our other tools seamlessly. They have accommodated most of our unique customisation requests, making it very user friendly for us to use."
Quality Assurance Manager
Mid-Market Pharma
"A user friendly and easy to go software. Finding old records is also a breeze, which definitely helps reduce time and makes the process more effective."
Nirogya D.
Dy. Manager
"System is compiled with 21 CFR Part 11 and EU Annex 11 compliance. The support from the team during the initial setup was really helpful and made the transition smooth."
Krishna C.
Compliance Lead
Built for the Most Regulated Industries
Deep domain expertise across the Life Sciences ecosystem, with purpose-built compliance frameworks for each vertical.
Pharmaceuticals
End-to-end batch manufacturing, quality control, and regulatory compliance for API and finished dosage plants.
Biotech
Flexible workflows for biologics manufacturing, cell line development, and biosimilar programs.
Medical Devices
ISO 13485-aligned quality systems, device history records, and CAPA management for Class I-III devices.
Gene & Cell Therapy
Specialized batch records, chain-of-custody tracking, and vein-to-vein traceability for advanced therapies.
CROs & CDMOs
Multi-client project management, flexible method validation, and rapid site onboarding for contract labs.
Nutraceuticals
Formulation management, stability studies, and regulatory filing support for dietary supplements and functional foods.
Real GxP Compliance Results from Real Pharma Clients
See how leading pharmaceutical companies transformed their operations with AmpleLogic.

Bharat Serum
60% Faster APQR Reports with Full Compliance
Bharat Serum transformed their annual product quality review process, replacing manual effort with automated, audit-ready report generation.
AmpleLogic automated what used to take our team weeks of manual compilation.

Cipla
Centralized User Access Across 15+ Sites
Cipla deployed centralized user access management across their global operations, ensuring data protection and continuous audit readiness.
A single platform for user access across all our manufacturing sites was a game-changer.

P&G
From Paper Logbooks to Fully Digital Operations
P&G eliminated paper-based logbooks entirely, moving to electronic logbooks across their manufacturing facilities with complete 21 CFR Part 11 compliance.
The transition from paper to digital was seamless — our operators adopted it in days.
Stop Managing 10 Pharma Solution Vendors. Start Running One 21 CFR Part 11 Compliant Life Sciences Platform.
Join 120+ pharmaceutical companies that have unified quality, lab, and manufacturing on AmpleLogic. See the difference in 30 minutes.
Or reach us directly at info@amplelogic.com · Toll free: 1800-2023-269
Stay Ahead in Life Sciences
Get the latest product updates, compliance news, and industry insights delivered to your inbox.